
Previously, we published a blog post on estimating hMSC lot sizes for clinical manufacturing, with the goal of outlining a development program that could tailor accordingly. This exercise is crucial because the calculated target cell lot size dictates the final production platform needed for your therapeutic product. The next step would be to determine the appropriate manufacturing platform, for each unit operation, that will meet the calculated hMSC lot sizes throughout clinical development. Having a solid, multi-year plan will help your company succeed at navigating this complex maze that is the path to market success.
 The final decision of production platforms can be overwhelming; even though there is a certain goal in mind for the present time, you do want to keep it flexible and scalable for other potential applications in the future. There is also the goal of managing through the “Comparability Challenges” as these changes are implemented. Adding to the complexity is that as the RegenMed industry grows, the technology providers of cell processing platforms across the various unit operations seems to be increasing in a fractal nature, with little standardization across devices. These technologies (e.g. bioreactors, continuous centrifuges, fill finish/controlled freezing, and other automation platforms) are significant investments to the company in the form of cost and time. It is the technologist’s and engineer’s jobs to drive the technology platform decision making process by derisking these technologies and establishing a multi-year development program, all while determining the costs associated with the program, and communicating these needs to the company’s business team so that they can raise the needed capital for these programs over time.
The final decision of production platforms can be overwhelming; even though there is a certain goal in mind for the present time, you do want to keep it flexible and scalable for other potential applications in the future. There is also the goal of managing through the “Comparability Challenges” as these changes are implemented. Adding to the complexity is that as the RegenMed industry grows, the technology providers of cell processing platforms across the various unit operations seems to be increasing in a fractal nature, with little standardization across devices. These technologies (e.g. bioreactors, continuous centrifuges, fill finish/controlled freezing, and other automation platforms) are significant investments to the company in the form of cost and time. It is the technologist’s and engineer’s jobs to drive the technology platform decision making process by derisking these technologies and establishing a multi-year development program, all while determining the costs associated with the program, and communicating these needs to the company’s business team so that they can raise the needed capital for these programs over time.
The goal of this post is to lay out the various scales of hMSC production and highlight the existing technology platforms for the different unit operations involved in the manufacturing process. This will help define the requirements that will guide the company’s multi-year process development program to meet projected future lot sizes.
Each phase of a clinical trial is associated with a specific production scale, which dictates the production platform
At the end of the last post, we arrived at the following estimated lot sizes based on a set of assumptions: 525 billion viable hMSCs per final commercial manufacturing lot, assuming a mid-range dose for a cardiac indication aimed to treat 100,000 patients per year, with a relatively safe, conservative assumptions regarding losses in cell viability and recovery during every step of the production process. Assuming a go-to-market lot size of 20% of the full commercial scale, we estimated that one could target a 100B cell lot size for Phase III, a 25B cell lot size for Phase II, and potentially a 10B cell lot size for a Phase I trial. These are simply guidelines that will change based on assumptions, but we recommend everyone go through this exercise (as outlined here) for each therapeutic program.

Traditional 2D hMSC manufacturing processes were capable of harvest densities of 20,000-30,000 cells/cm2 [1]. Starting with a working cell bank of 40M cells, the Phase I lot size could be achieved using 60-80 2D CellStacks at this range of harvest density. High productivity hMSC Bioprocess systems such as RoosterBio’s drive cell density at harvest to ≥ 40,000 cells/cm2, while maintaining low cumulative PDL of ~16-18. The actual 2D harvest numbers can be > 60,000 cells/cm2 (this is mostly donor dependent), however downstream processing losses typically bring the numbers back down [2], so we’d like to do all our calculations with a conservative density of 40,000 cells/cm2. This higher harvest density decreases the number of CellStacks to ~40 compared to traditional 2D planar manufacturing processes for this Phase I scale, reducing process complexity, labor and overall COGS significantly. Harvest processing time can be reduced by several hours and the facility footprint by hundreds of square feet, including many expensive reagents costs such as media, harvest reagent, etc. With these numbers, the processes can be developed and executed quickly in a robust 10-layer CellStack/CellFactory process, therefore getting a final hMSC product into Phase I for a proof to therapy with a low-risk process. Achieving a rapid and low cost Phase I feasibility is usually the best path for pharmaceutical development, and thus drives much of the 2D platform decisions for hMSC products. We do help our customers rapidly implement these processes via our Process Design and Acceleration Services.
Scalable hMSC clinical manufacturing needs movement away from 2D planar platforms
Each manufacturing phase leading up to the go-to-market lot size is associated with a new scale of production, thus requiring a scale-up development program. Process development programs are time-consuming and expensive, therefore justifying the necessity of a multi-year planning for efficient capital utilization within a company. Specific time-intensive planning aspects to proactively address include budgeting for at least 6 months of disposable engineering (having each single use bag and disposable at each unit operation with compatible connections), and then planning for at least 3-6 half scale runs and 3 full scale runs to understand and work out kinks in a full process prior to undertaking tech transfer. This can easily encompass up to 12-18 months of development studies for each scale-up program.
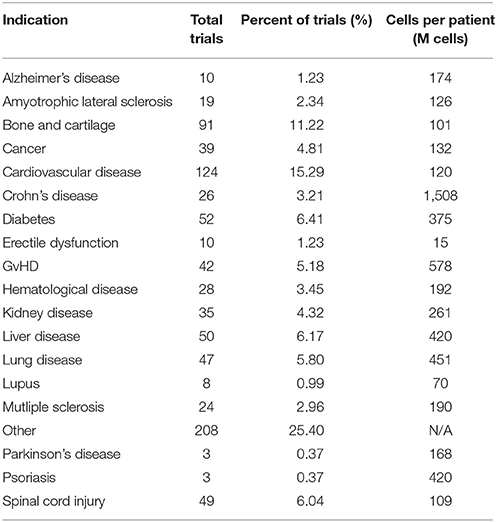
The scale of production at our proposed Phase II lot size of 25B is challenging to achieve using 2D planar platforms, even with high productivity systems. Assuming a typical harvest yield of 40,000 cells/cm2, 25B cells in CS10’s requires ~100 CellStacks. There are several challenges with this; it is very expensive, time consuming, labor intensive, and not environmentally friendly (think of the >800 sq ft footprint that the CellStacks occupy and how much plastic that is). The largest 2D planar platform, the automated 120-layer hyperstacks, can generate ~100B lot size, however there is no option of scaling-up from there. At scales larger than 15-20 Billion cells/lot, we recommend moving directly to 3D bioreactor platforms to maintain scalability for the future. We estimate that a 100B target lot size is relevant for ~95% of the indications requiring hMSC treatment based off of our analysis of cell dose from the ClinicalTrials.gov website [3], with some exceptions including low dose indications such as ocular diseases [4]. Therefore, we recommend a jump to a bioreactor production platform for most development programs aiming to get to Phase II.
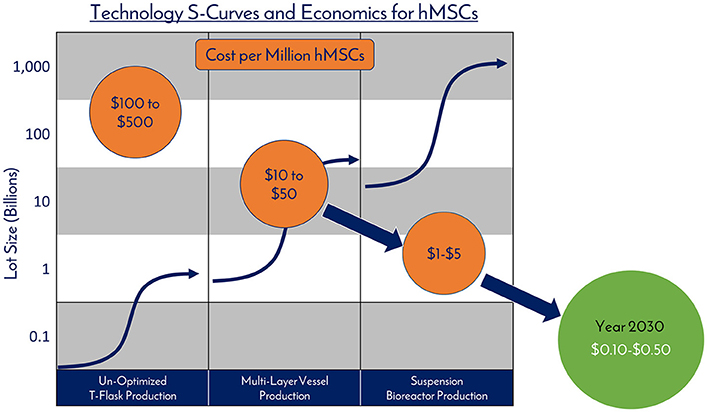
As the field moves into suspension bioreactors from 2D, there are new opportunities for productivity gains during production. Borrowing from best practices in the monoclonal antibody field, fed batch processes can lead to high media productivity, and we have established this in hMSC production as well. With a fed batch process, coupled with well QC’d, low PDL cell banks, it is routine to achieve a range of final cell yields of 0.4M - 0.8M cells/ml in a microcarrier suspension bioreactor process incorporating a bioreactor feed, when performed in a low-shear Vertical-Wheel™ bioreactor. A 3D fed-batch process increases media usage efficiency by >2 times compared to our 2D batch systems (or by >15 times compared to a traditional hMSC 2D flask culture), thus simplifying the overall process, increasing cell productivity, and reducing media costs per cell produced. It is these compounded efficiencies that will drive the cell cost curve down with further scale advancements.
For estimating bioreactor production volumes, we assume a conservative average bioreactor yield of 0.5M cells/ml (again, this is donor dependent, among other variables). Thus, a production vessel of 50L bioreactor is required for a 25B cell lot size; the 100B hMSC go-to-market lot size requires a 200L bioreactor, and the full-scale production requires a 1000L bioreactor. To achieve these lot sizes while maintaining the PDL of the final product (a critical quality attribute of every hMSC final product), the working cell bank must scale in size with the process, and will range from 100M to 2B (in closed, single use formats).

Proactively addressing downstream processing bottlenecks
The subsequent post-harvest processing steps involve unit operations which rely on the scale of the expansion platform [2], therefore it is critical to proactively address downstream process unit operations as you choose your expansion technologies. You don’t want to manufacture your products at a scale only to waste a large fraction of it due to incapability to process. Cell harvesting from the bioreactor is immediately followed by a cell-microcarrier separation process. While there are no standard accepted criteria for the amount of microcarriers that can be in the final product, near complete removal of microcarriers from the cell therapy product is critical in ensuring safety for the patient. For the microcarrier removal unit operation, screen-based depth filtration technology has been implemented, trapping microcarriers within 60-100 µm meshes while letting cells pass through. This leaves the cells in the quenched harvest reagent for further clarification and concentration. Alternatively, the development and use of dissolvable microcarriers in large scale hMSC bioreactor culture could potentially eliminate the need for a separation unit, creating a more streamlined, simplified hMSC manufacturing process.

The microcarrier-free cell suspension coming out of the separation step goes into a volume reduction / wash operation. Large scale production of hMSCs (starting at Phase II) demands scalable technologies for this step, i.e. tangential flow filtration (TFF) or continuous counterflow centrifugation system [2] such as kSep (Sartorius) and Rotea (Scinogy). Newer technologies such as acoustic wave separation technology (e.g. Pall’s Cadence™ Acoustic Separator, FloDesign Sonics) are also being developed and optimized for hMSC manufacturing process. With 100B lot size, the kSep is the only platform today that can accommodate 200L volume within a reasonable manufacturing timescale (to give a rough idea, our experience of processing of 60L of 0.4M cells/ml in the kSep400 with conservative process parameters takes about 1.5 hours in one single cycle, while a typical open centrifugation system for this volume would have taken over 3 hours in 30 consecutive cycles). At 500B cells, the kSep6000S is the only platform that could potentially process the volume associated with this full commercial scale lot size. Other volume reduction technologies such as Rotea or FloDesign Sonics’ Acoustic Wave Technology can be implemented in productions associated with earlier phases or indications associated with smaller lot sizes due to their smaller processing capabilities (10-50B cells), however keep in mind that these technologies might scale in the future for hMSC manufacturing. Studies can also be done to test these systems for a combined separation / concentration step during the manufacturing steps, but this will require extensive process development and validation for use with cell/microcarrier suspensions.
The envisioned format of the final cell product is a pharma-style vial with ~75M cells/vial at 10 ml fill. To fill 10B cells, a semi-automated vialing system can be used such as the M1 Filling Station (Aseptic Technologies). For the full scale production at 500+ vials/hr, a fully automated vialing system such as the Crystal® L1 Robot Line can be employed.
Cryopreservation, followed by storage, is the last step of the manufacturing process. Since fast, controlled rate freezing process is critical in maintaining cell health, large-scale cryopreservation platforms such as the CryoMed™ Controlled Rate Freezers (CRF) which allows a custom user-defined recipe is commonly used. Each process development group will work to optimize a controlled rate freezer recipe that works for their final products, with post-thaw viability and expansion being the performance metric.
After all processes, it is important to verify the final cell product quality. The safety of the cells needs to remain intact and critical quality attributes of the cells need to be maintained. RoosterBio performs a general analytic panel to ensure safety and critical quality attributes of hMSCs (including cell performance, identity, and functionality testing), but each final product will have its unique testing requirements and must be performed within the context of each development program. However, our goal is to identify and derisk the comparability challenges for our customers prior to them scaling, simplifying and accelerating the process and product development for each intended program.
In conclusion, we have highlighted various existing technology platforms involved in an hMSC manufacturing process. You can think of this exercise as a decision-making tool to help streamline an hMSC clinical manufacturing program. As this informs the development team on the unit operation choices associated with each phase, it also helps the team define their requirements and invest in lot-size-appropriate technologies. This leads to a RegenMed company’s multi-year planning of its process development program to meet the peak commercial demands for most indications requiring hMSC treatment.
If you have an interest in discussing scalable production platforms, evaluating our complete solutions that radically simplify hMSC process development, or are interested in our Process Design & Acceleration Services, please reach out to us at info@roosterbio.com, or simply comment on this blog post!
References:
“It is the technologist’s and engineer’s jobs to drive the technology platform decision making process”

The goal of this post is to lay out the various scales of hMSC production and highlight the existing technology platforms for the different unit operations involved in the manufacturing process. This will help define the requirements that will guide the company’s multi-year process development program to meet projected future lot sizes.
Each phase of a clinical trial is associated with a specific production scale, which dictates the production platform
At the end of the last post, we arrived at the following estimated lot sizes based on a set of assumptions: 525 billion viable hMSCs per final commercial manufacturing lot, assuming a mid-range dose for a cardiac indication aimed to treat 100,000 patients per year, with a relatively safe, conservative assumptions regarding losses in cell viability and recovery during every step of the production process. Assuming a go-to-market lot size of 20% of the full commercial scale, we estimated that one could target a 100B cell lot size for Phase III, a 25B cell lot size for Phase II, and potentially a 10B cell lot size for a Phase I trial. These are simply guidelines that will change based on assumptions, but we recommend everyone go through this exercise (as outlined here) for each therapeutic program.

Each manufacturing phase leading up to the go-to-market lot size is associated with a new scale of production, thus requiring a scale-up development program. Process development programs are time-consuming and expensive, therefore justifying the necessity of a multi-year planning for efficient capital utilization within a company. Specific time-intensive planning aspects to proactively address include budgeting for at least 6 months of disposable engineering (having each single use bag and disposable at each unit operation with compatible connections), and then planning for at least 3-6 half scale runs and 3 full scale runs to understand and work out kinks in a full process prior to undertaking tech transfer. This can easily encompass up to 12-18 months of development studies for each scale-up program.
The scale of production at our proposed Phase II lot size of 25B is challenging to achieve using 2D planar platforms, even with high productivity systems. Assuming a typical harvest yield of 40,000 cells/cm2, 25B cells in CS10’s requires ~100 CellStacks. There are several challenges with this; it is very expensive, time consuming, labor intensive, and not environmentally friendly (think of the >800 sq ft footprint that the CellStacks occupy and how much plastic that is). The largest 2D planar platform, the automated 120-layer hyperstacks, can generate ~100B lot size, however there is no option of scaling-up from there. At scales larger than 15-20 Billion cells/lot, we recommend moving directly to 3D bioreactor platforms to maintain scalability for the future. We estimate that a 100B target lot size is relevant for ~95% of the indications requiring hMSC treatment based off of our analysis of cell dose from the ClinicalTrials.gov website [3], with some exceptions including low dose indications such as ocular diseases [4]. Therefore, we recommend a jump to a bioreactor production platform for most development programs aiming to get to Phase II.
{kind=link}
As the field moves into suspension bioreactors from 2D, there are new opportunities for productivity gains during production. Borrowing from best practices in the monoclonal antibody field, fed batch processes can lead to high media productivity, and we have established this in hMSC production as well. With a fed batch process, coupled with well QC’d, low PDL cell banks, it is routine to achieve a range of final cell yields of 0.4M - 0.8M cells/ml in a microcarrier suspension bioreactor process incorporating a bioreactor feed, when performed in a low-shear Vertical-Wheel™ bioreactor. A 3D fed-batch process increases media usage efficiency by >2 times compared to our 2D batch systems (or by >15 times compared to a traditional hMSC 2D flask culture), thus simplifying the overall process, increasing cell productivity, and reducing media costs per cell produced. It is these compounded efficiencies that will drive the cell cost curve down with further scale advancements.
{kind=link}
For estimating bioreactor production volumes, we assume a conservative average bioreactor yield of 0.5M cells/ml (again, this is donor dependent, among other variables). Thus, a production vessel of 50L bioreactor is required for a 25B cell lot size; the 100B hMSC go-to-market lot size requires a 200L bioreactor, and the full-scale production requires a 1000L bioreactor. To achieve these lot sizes while maintaining the PDL of the final product (a critical quality attribute of every hMSC final product), the working cell bank must scale in size with the process, and will range from 100M to 2B (in closed, single use formats).
Table 1. Summary of technology landscape for allogeneic hMSC manufacturing – by unit operation

The subsequent post-harvest processing steps involve unit operations which rely on the scale of the expansion platform [2], therefore it is critical to proactively address downstream process unit operations as you choose your expansion technologies. You don’t want to manufacture your products at a scale only to waste a large fraction of it due to incapability to process. Cell harvesting from the bioreactor is immediately followed by a cell-microcarrier separation process. While there are no standard accepted criteria for the amount of microcarriers that can be in the final product, near complete removal of microcarriers from the cell therapy product is critical in ensuring safety for the patient. For the microcarrier removal unit operation, screen-based depth filtration technology has been implemented, trapping microcarriers within 60-100 µm meshes while letting cells pass through. This leaves the cells in the quenched harvest reagent for further clarification and concentration. Alternatively, the development and use of dissolvable microcarriers in large scale hMSC bioreactor culture could potentially eliminate the need for a separation unit, creating a more streamlined, simplified hMSC manufacturing process.

The envisioned format of the final cell product is a pharma-style vial with ~75M cells/vial at 10 ml fill. To fill 10B cells, a semi-automated vialing system can be used such as the M1 Filling Station (Aseptic Technologies). For the full scale production at 500+ vials/hr, a fully automated vialing system such as the Crystal® L1 Robot Line can be employed.
Cryopreservation, followed by storage, is the last step of the manufacturing process. Since fast, controlled rate freezing process is critical in maintaining cell health, large-scale cryopreservation platforms such as the CryoMed™ Controlled Rate Freezers (CRF) which allows a custom user-defined recipe is commonly used. Each process development group will work to optimize a controlled rate freezer recipe that works for their final products, with post-thaw viability and expansion being the performance metric.
After all processes, it is important to verify the final cell product quality. The safety of the cells needs to remain intact and critical quality attributes of the cells need to be maintained. RoosterBio performs a general analytic panel to ensure safety and critical quality attributes of hMSCs (including cell performance, identity, and functionality testing), but each final product will have its unique testing requirements and must be performed within the context of each development program. However, our goal is to identify and derisk the comparability challenges for our customers prior to them scaling, simplifying and accelerating the process and product development for each intended program.
In conclusion, we have highlighted various existing technology platforms involved in an hMSC manufacturing process. You can think of this exercise as a decision-making tool to help streamline an hMSC clinical manufacturing program. As this informs the development team on the unit operation choices associated with each phase, it also helps the team define their requirements and invest in lot-size-appropriate technologies. This leads to a RegenMed company’s multi-year planning of its process development program to meet the peak commercial demands for most indications requiring hMSC treatment.
If you have an interest in discussing scalable production platforms, evaluating our complete solutions that radically simplify hMSC process development, or are interested in our Process Design & Acceleration Services, please reach out to us at info@roosterbio.com, or simply comment on this blog post!
- Rowley et al., 2012. Meeting Lot-Size Challenges of Manufacturing Adherent Cells for Therapy. BioProcess International 10(3): 16-22
- Pattasseril et al., 2013. Downstream Technology Landscape for Large-Scale Therapeutic Cell Processing. BioProcess International 11(3): 38-47
- Olsen et al., 2018. Peak MSC—Are We There Yet? Front Med 5:178. doi: 10.3389/fmed.2018.00178
- Simaria et al., 2013. Allogeneic cell therapy bioprocess economics and optimization: Single‐use cell expansion technologies. Biotechnol Bioeng 111(1): 69-83. doi: 10.1002/bit.25008
No comments:
Post a Comment
All comments are welcome, but we do not support hateful or lewd messages. Please make your comments professional and in the spirit of adding to the scientific discussion!